The good ole way of accessing the subclavian vein
Subclavian Puncture
Subclavian Puncture
This is a variation of the technique used by anesthetists to access the subclavian vein. The anesthetists approach the vein starting high up in the delto-pectoral groove aiming along the clavicular shaft – this makes the skin puncture site near the clavicle but we need it further below at the top of the future pacemaker pocket.
Therefore the skin puncture is done as shown at the hollow of the delto-pectoral triangle, about 1-2 finger-breadths below from the clavicle at its junction between the middle third and lateral third (roughly at its “bend”). It should be realized that the needle will be traveling through the upper aspect of the pectoralis major muscle (through its clavicular head)
The puncture needle is slowly advanced towards the shaft of the clavicle (at about an 20-30 degree angle to the skin) and once it hits the clavicle, the needle is slightly withdrawn and angulated (increased angle of attack to skin surface ) more so that the tip is under the clavicle. Then, the direction of the needle is changed so that now the tip aims towards the supra-sternal notch. The needle is slowly advanced in that direction (now at a skin angle of 20 – 30 degrees) with gentle suction to see whether it punctures the vein – whence dark venous blood would be aspirated. Once blood is aspirated, the needle is steadied and liberal aspiration of blood is done to ensure good access in to the vein. Thereafter the syringe is removed and guide-wire advanced in to the lumen.
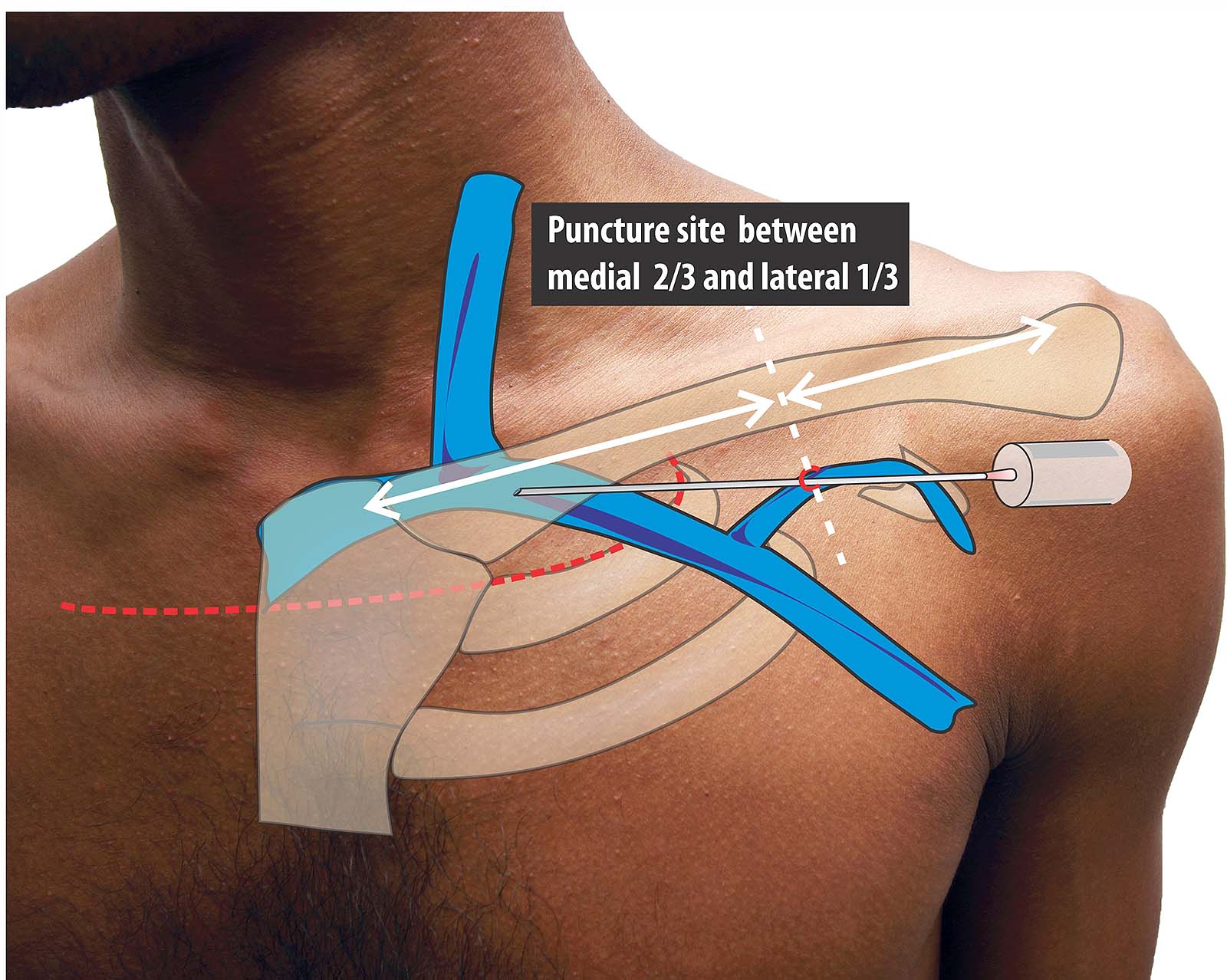
Figure : Schematic of final approach to the subclavian vein. This is the final approach to the subclavian vein. (See text above and guide below for more details). Subclavian puncture is relatively straightforward from easiness of venous access. But it has its share of problems and extra-thoracic subclavian / axillary vein puncture is the recommended technique to master.
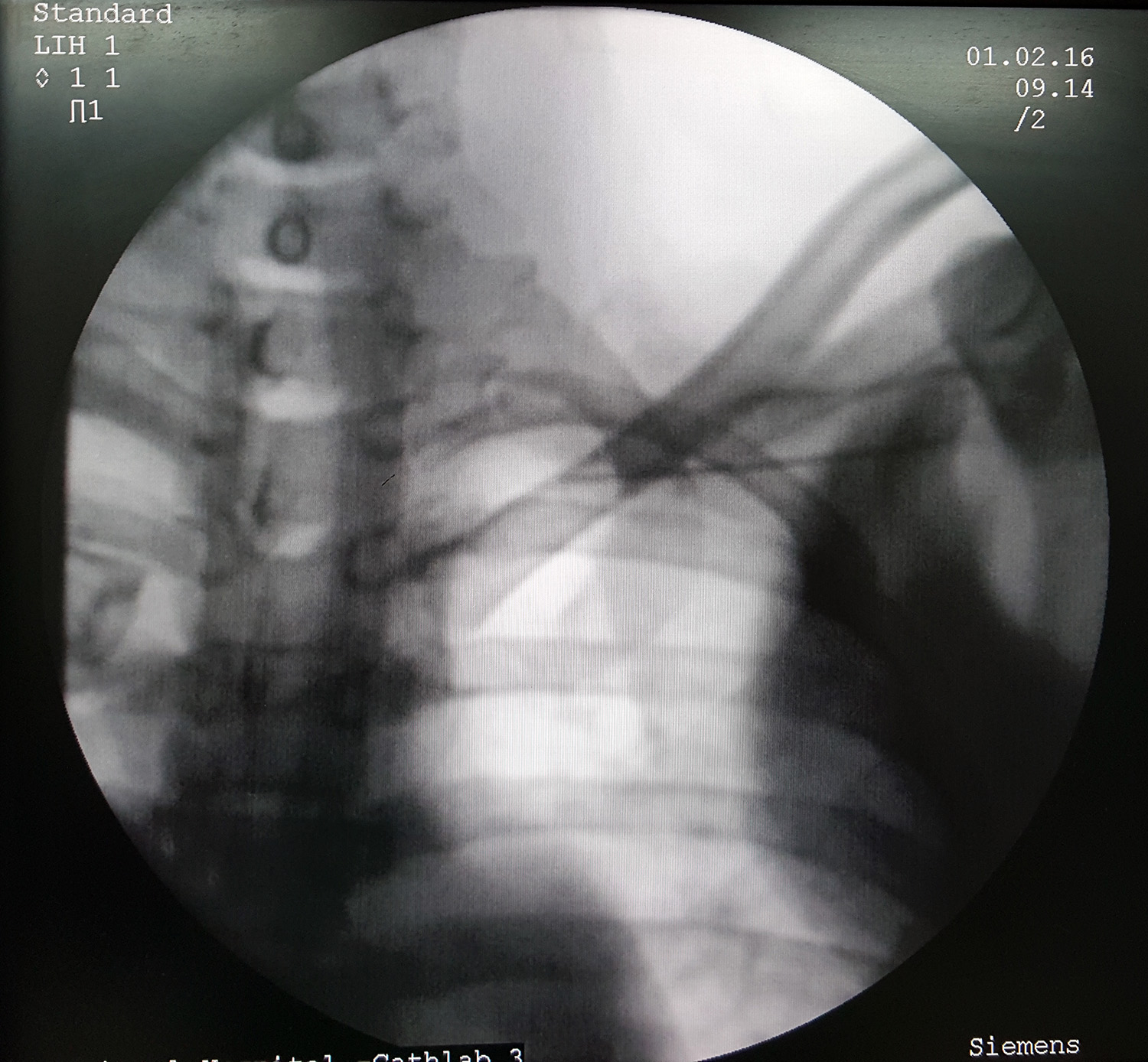
Figure : Fluroscopic position of needle during subclavian access. Note that the needle tip is well medial to the first rib and under the clavicle. Also note the operators hand shadow on the fluro field indicting that the syringe would have need steadying very medially. (This case was a difficult puncture and had to be attempted in this way)
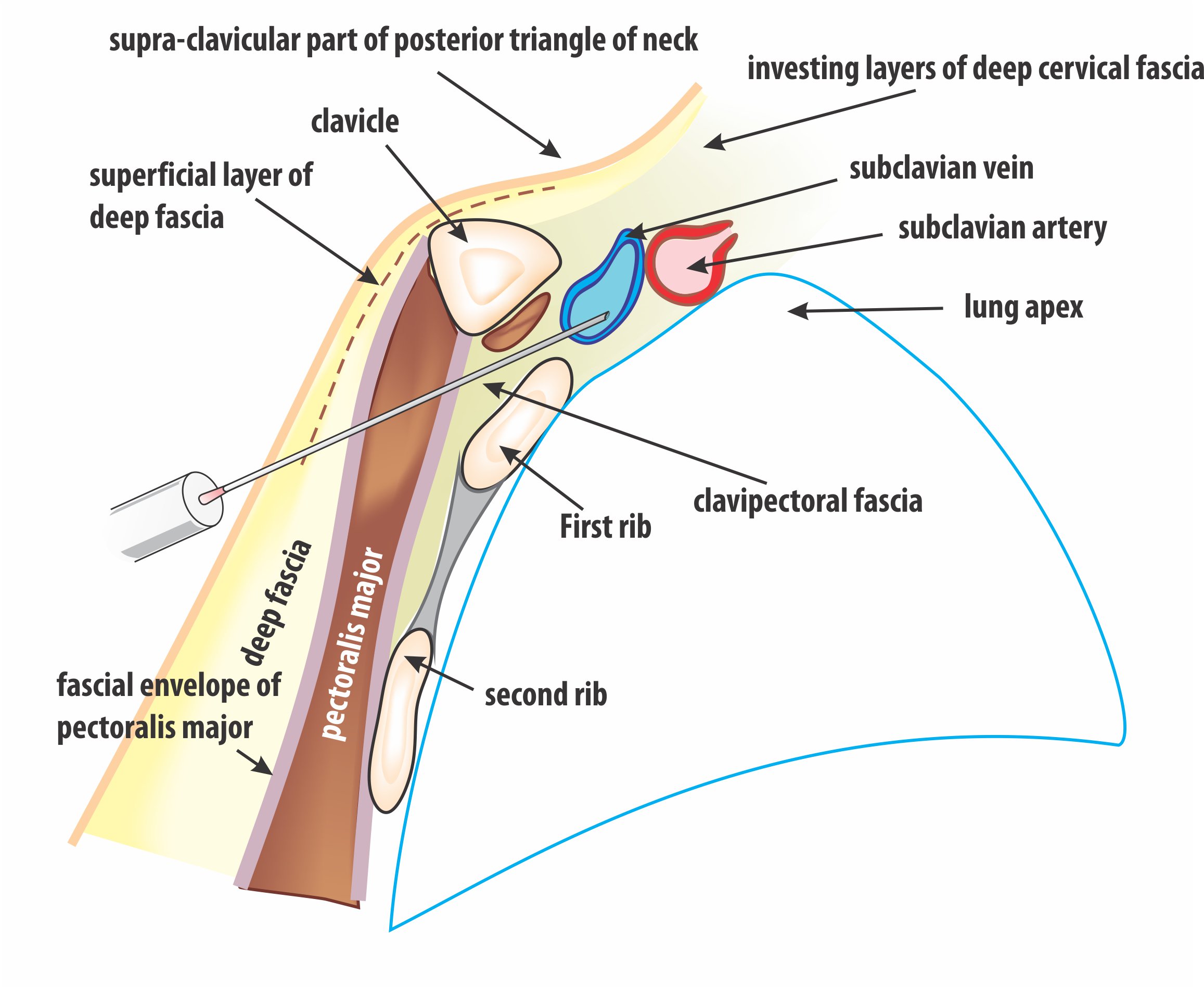
Figure : The anatomic pathway of subclavian venous puncture. As depicted the needle travels between the clavicle and the first rib to reach the vein and at this point the vein overlies the lung apex. It can be appreciated how close the needle is to the lung and how easily a needle may penetrate the lung apex if pushed too far. (The axillary vein is not visible in this cut-plane as it is more towards the viewer and out of the first rib border)
Subclavian Puncture Steps :

Check the needle attachment to the syringe. Needle should be loosely attached to a non-luer lock syringe. (If the attachment is too tight, you may loose access while struggling to release the syringe)

The hollow of the deltopectoral triangle is palpated at 1 – 2 finger-breadths below the junction of the lateral third and middle third of the clavicle. Needle enters the skin here.
The needle is advanced at a skin angle of 30 degrees, towards the clavicular shaft.
Once the needle tip hits the bone, the needle is slightly withdrawn and the angle of attack is increased as to enter the underside of the clavicle. As soon as one feels the underside of the clavicle, advancement should be stopped and direction of the needle change to point towards the supra-sternal notch.

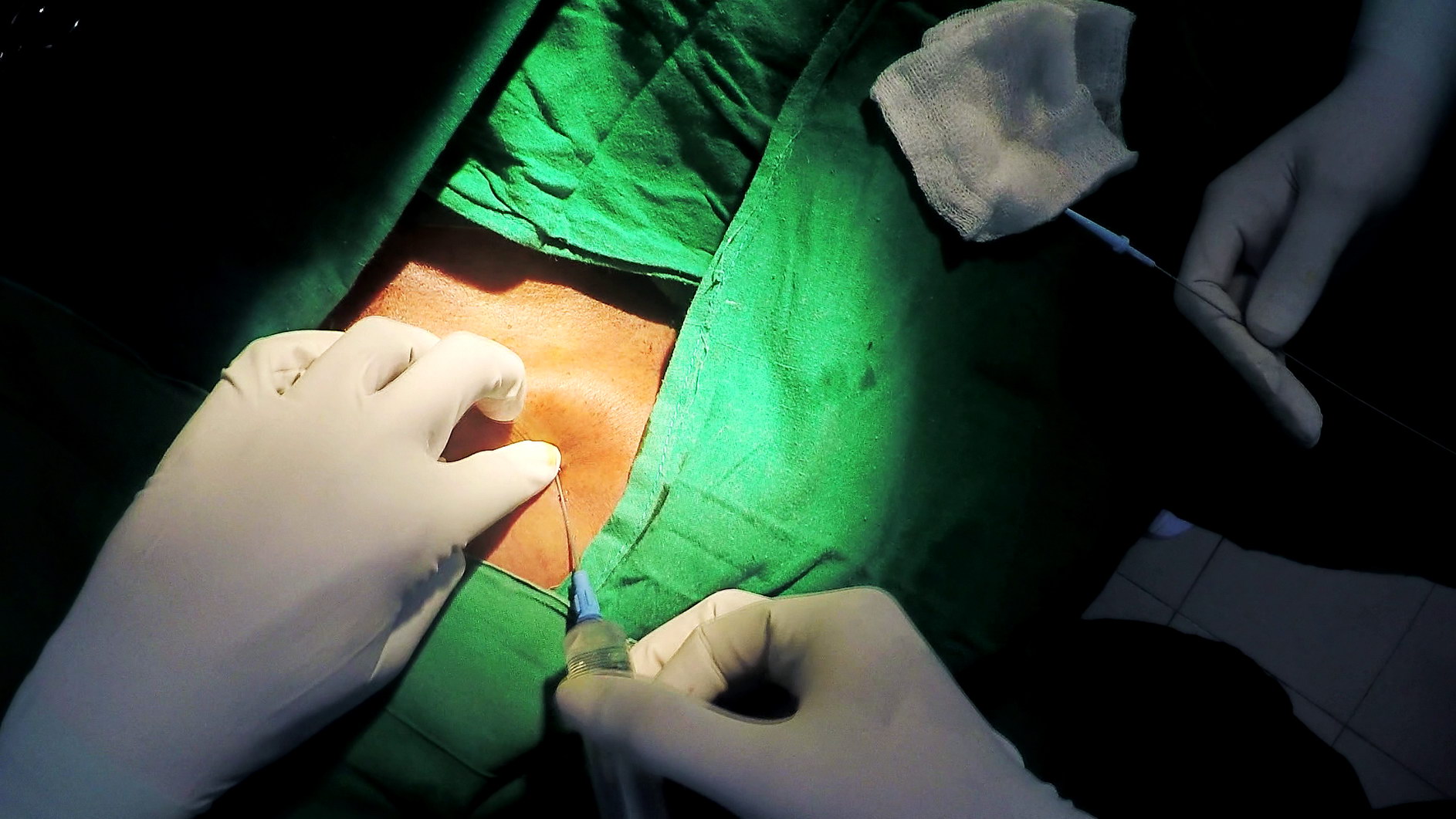
Now the needle is advanced in the direction of the supra-sternal notch. (operators’ left index finger is at the supra-sternal notch) Note : A fairly long length of the needle may be needed to reach the vein
Gentle suction is applied as the needle is advanced. (Vigorous suction should be avoided as it will draw fat / muscle debris in to the lumen and obstruct it)

At one point one will enter the vein and blood will be visible in the syringe with suction.A generous amount of blood should be aspirated to confirm venous access.
If the vein is not accessed despite full advancement of the needle, one can try sight variation in depth of penetration. However, the risk of pneumothorax is high in this region and it is recommended that an alternative x-ray guided approach be used.
Recommended reading